
Appetite pathway peptides: Science, benefits, and use

TL;DR:
- Appetite regulation involves multiple signals from the gut and brain, with peptides like ghrelin, PYY, GLP-1, and LEAP2 playing key roles. Emerging peptides such as semaglutide, tirzepatide, and retatrutide significantly enhance weight loss by targeting these pathways and modifying food reward mechanisms. Combining these peptides and understanding their biological effects can optimize treatment, but sustainable results rely on integrating lifestyle changes alongside pharmacological interventions.
Hunger isn’t a character flaw. If you’ve ever blamed yourself for caving on a diet, the real story is far more interesting than willpower. Your body runs a sophisticated biological negotiation between your gut, your brain, and a cast of molecular messengers that decide when you eat, how much, and how urgently. Appetite pathway research peptides are now giving scientists and fitness-focused individuals a way to intervene in that negotiation at a mechanistic level, targeting the exact receptors and signals that drive cravings. This guide breaks down how these peptides work, what the latest evidence says, and what it actually means for your performance and weight management goals.
Table of Contents
- How appetite pathways and peptides regulate hunger
- Key appetite pathway research peptides: Evidence and mechanisms
- GLP-1, PYY, and beyond: Combination strategies for optimal results
- Practical applications and real-world considerations
- The uncomfortable truth about appetite peptide breakthroughs
- Explore appetite research peptides and expert fitness solutions
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Peptides target appetite | Research peptides influence key hunger and satiety pathways for advanced appetite control. |
| Clinical evidence supports use | Trials show significant weight loss and appetite reduction, even for genetic obesity cases. |
| Combination strategies work best | Combining GLP-1, PYY, and similar peptides may maximize appetite suppression and minimize side effects. |
| Supplements aren’t substitutes | OTC options lack the effectiveness of research peptides like semaglutide or tirzepatide. |
| Expert guidance is crucial | Safe, effective use of appetite pathway peptides requires medical oversight and personalized strategies. |
How appetite pathways and peptides regulate hunger
Appetite regulation isn’t one switch. It’s a layered system involving both central pathways in the brain and peripheral signals from the gut, pancreas, and adipose tissue. The hypothalamus acts as the command center, integrating signals from circulating peptides to either ramp up hunger or shut it down. When you understand this system, you stop thinking about cravings as weakness and start seeing them as chemistry.
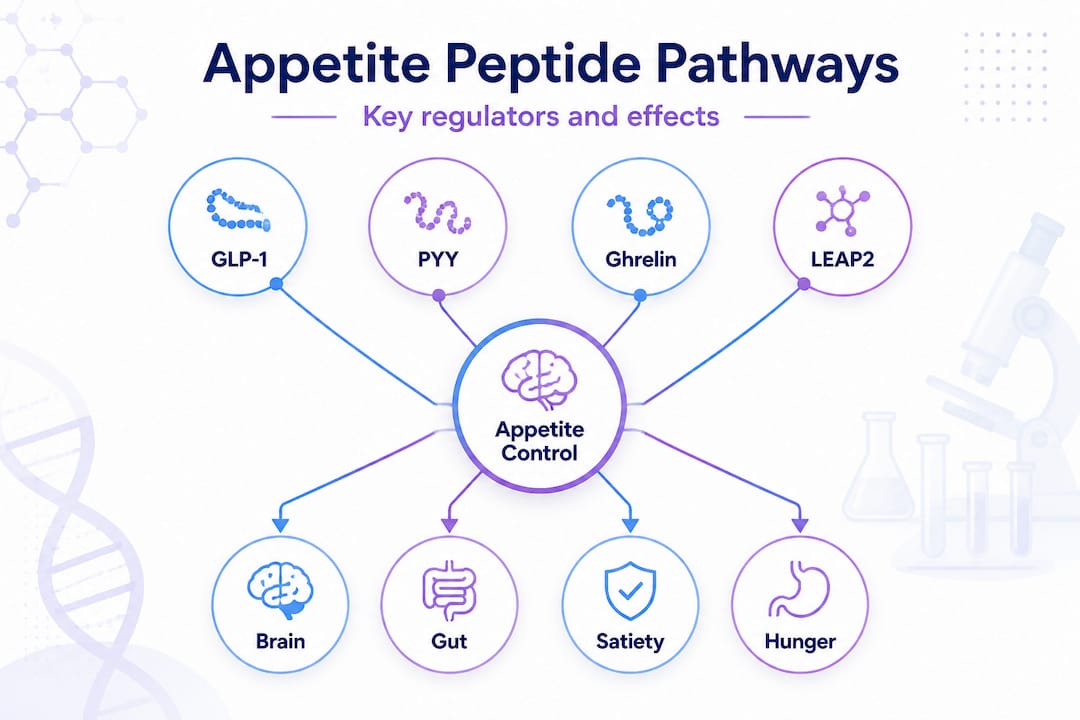
The four peptides you need to know first are ghrelin, PYY, GLP-1, and LEAP2. Each plays a distinct role in this system, and each represents a potential target for intervention.
| Peptide | Primary function | Site of action | Effect on appetite |
|---|---|---|---|
| Ghrelin | Stimulates hunger | Stomach, hypothalamus | Increases food intake |
| PYY3-36 | Suppresses appetite | Gut, hypothalamus Y2 receptors | Reduces food intake |
| GLP-1 | Promotes satiety, slows gastric emptying | Gut, brain, pancreas | Decreases hunger |
| LEAP2 | Blocks ghrelin signaling | GHSR1a receptors | Reduces hunger drive |
Ghrelin, acylated by GOAT, acts as an orexigenic (hunger-promoting) peptide via GHSR1a receptors, while LEAP2 acts as its antagonist, with both peptide levels shifting significantly after bariatric surgery. Meanwhile, PYY3-36 suppresses appetite via Y2 receptors in the hypothalamus, reduces food intake, delays gastric emptying, and improves insulin sensitivity.
These peptides don’t operate in isolation. They respond dynamically to what you eat, how much you exercise, and your current body weight. Here’s how:
- Caloric restriction raises ghrelin and lowers PYY, making hunger more intense over time
- High-intensity exercise temporarily suppresses ghrelin while boosting PYY and GLP-1
- Weight loss consistently elevates ghrelin, which is one key reason rebound hunger is so powerful
- High-protein meals produce stronger PYY and GLP-1 responses than high-carb meals
- Gut microbiome health influences how effectively peripheral peptides are produced and signaled
Understanding the role of bioactive peptides benefits in this system helps explain why diet quality matters beyond just calories. The type of food you eat shapes the peptide environment your brain is working with.
Pro Tip: Not all hunger is peptide-driven. Habit-driven hunger, triggered by time of day, boredom, or environmental cues, operates through a different neural circuit. If you’re eating at the same time every day regardless of actual hunger signals, that’s behavioral, not biochemical. Distinguishing the two helps you target the right intervention.
Key appetite pathway research peptides: Evidence and mechanisms
With these pathways in mind, let’s spotlight breakthrough peptides and examine their latest clinical evidence. The research landscape has accelerated dramatically, with several molecules now showing effects that would have seemed implausible five years ago.
| Peptide | Target mechanism | Route | Average weight loss | Additional effects |
|---|---|---|---|---|
| Semaglutide | GLP-1 receptor agonist | Subcutaneous injection | 15 to 17% body weight | Cardiovascular protection |
| Tirzepatide | GLP-1 and GIP dual agonist | Subcutaneous injection | 20 to 22% body weight | Improved insulin sensitivity |
| Retatrutide | GLP-1, GIP, glucagon triple agonist | Subcutaneous injection | Up to 24% body weight | Enhanced fat oxidation |
| PYY3-36 | Y2 receptor agonist | Intranasal or injection | Moderate (adjunct) | Reduced meal size, delayed gastric emptying |
| LEAP2 | Ghrelin receptor antagonist | Research stage | Investigational | Blocks hunger signaling post-surgery |
The weight loss numbers are striking. Tirzepatide and semaglutide reduce body weight in MC4R knockout mice by 19.7% and 31.6% over 21 days, demonstrating efficacy even in genetic appetite pathway deficiencies where standard interventions typically fail. That’s a significant finding because MC4R mutations account for a meaningful percentage of severe obesity cases in humans.
The mechanism isn’t just “feeling less hungry.” It’s more precise than that. Tirzepatide reduces energy intake by 524.6 kcal at week 3 versus placebo in a phase 1 trial, simultaneously decreasing appetite, cravings, and hunger while altering brain reactivity to high-fat, high-sugar foods. That last point matters enormously. These peptides don’t just reduce how hungry you feel. They change how rewarding food looks to your brain.
Here’s the step-by-step mechanism from injection to neurological impact:
- Peptide is administered via subcutaneous injection, entering systemic circulation
- Peripheral binding occurs at gut receptors (GLP-1R, GIPR), slowing gastric emptying and reducing nutrient absorption rate
- Vagal nerve signaling carries satiety information from gut to brainstem
- Hypothalamic integration occurs as the peptide crosses the blood-brain barrier or acts via circumventricular organs
- Reward pathway modulation reduces dopaminergic response to high-calorie food cues
- Net behavioral effect is reduced meal size, longer time between meals, and lower cravings for hyper-palatable foods
From landmark 2026 research: Tirzepatide’s dual GLP-1 and GIP mechanism produces appetite suppression and metabolic improvement that exceeds either pathway targeted alone. Retatrutide’s triple agonism pushes weight loss even further, with trial participants showing up to 24% total body weight reduction over 48 weeks. These figures represent a categorical shift from what was previously achievable with pharmacological intervention.
For a deeper technical breakdown of how these molecules work across performance contexts, the peptide guide for performance covers the mechanistic science in detail. If you’re evaluating whether these tools are appropriate for your goals, prescription peptides for weight loss outlines the regulatory and clinical framework you need to understand first.
GLP-1, PYY, and beyond: Combination strategies for optimal results
Not all peptides act solo. Researchers are increasingly exploring combination strategies that target multiple appetite pathways simultaneously, aiming to amplify results while reducing the dose-dependent side effects that come from pushing a single agent hard.
The logic is straightforward. GLP-1 and PYY operate through distinct receptors and complementary mechanisms. GLP-1 analogs work independently of MC4R, which means they remain effective even in individuals with genetic obesity where the melanocortin pathway is compromised. PYY complements GLP-1 for multi-target therapy, with combinations showing synergistic appetite suppression without direct insulinotropic (insulin-stimulating) effects, which reduces hypoglycemia risk.
Combination trials are showing results that single-agent studies can’t match. Tirzepatide’s dual mechanism already outperforms semaglutide in head-to-head comparisons, and retatrutide’s triple agonism pushes the ceiling further. The pattern is consistent: more pathway coverage equals more robust appetite suppression.
Benefits of combination peptide strategies include:
- Enhanced appetite suppression through multiple receptor systems working simultaneously
- Improved metabolic profile including better lipid control, insulin sensitivity, and blood pressure
- Reduced single-agent side effects because lower doses of each peptide can be used
- Greater durability of weight loss due to multiple compensatory mechanisms being addressed
- Broader applicability across different genetic obesity subtypes
The pitfalls are real, though. Combining peptides without proper medical oversight introduces risks that aren’t well characterized in long-term data. Overlapping gastrointestinal side effects can compound significantly. Unproven supplement combinations marketed as “GLP-1 stacks” online have no clinical backing and may interact with legitimate therapies in unpredictable ways.
For a clear-eyed look at what’s supported versus what’s hype, peptide safety and benefits provides a grounded framework. If you’re thinking about optimizing how peptides are absorbed and utilized, the peptide bioavailability guide addresses the practical variables that affect real-world outcomes.
Pro Tip: If you’re already on a GLP-1 agonist and considering adding another appetite-modulating agent, track your side effect profile week by week. Nausea, fatigue, and appetite suppression can stack unpredictably, and what feels manageable at week two may become unsustainable at week six. Document everything and review with a prescribing physician before adding anything.
Practical applications and real-world considerations
Armed with scientific understanding, here’s what practical use, safety, and limitations look like in real life. The gap between clinical trial data and everyday application is wider than most fitness content acknowledges.

These peptides are primarily accessed through prescription channels for clinical obesity management, though research contexts and emerging compounding pharmacy markets have expanded access. The fitness community’s interest is growing rapidly, but so is the misinformation surrounding it.
Steps to assess whether research peptides are a fit for your goals:
- Medical screening including metabolic panel, thyroid function, cardiovascular baseline, and BMI assessment
- Expert consultation with an endocrinologist or obesity medicine specialist who understands the current evidence base
- Legal status verification in your jurisdiction, as compounded semaglutide and tirzepatide regulations vary significantly by country and state
- Baseline monitoring of weight, body composition, energy intake, and relevant biomarkers before starting
- Ongoing tracking of both efficacy and side effects at regular intervals, with dose adjustments guided by clinical response
The supplement market has moved aggressively to capitalize on GLP-1 awareness. Over-the-counter GLP-1 mimicking supplements lack the efficacy of pharmaceutical peptides like semaglutide, with alternatives like berberine yielding only approximately 4 lbs of weight loss in studies. That’s not nothing, but it’s a fraction of what clinical peptides produce, and it doesn’t justify the premium pricing many brands charge.
Side effects and practical considerations to keep in mind:
- Gastrointestinal symptoms including nausea, vomiting, and constipation are the most common, especially during dose escalation
- Muscle mass loss can occur alongside fat loss if protein intake and resistance training aren’t prioritized
- Mood and libido changes are increasingly documented, as GLP-1 agonists may decrease sexual desire via serotonergic pathways
- Rebound weight gain is common after discontinuation without sustained lifestyle changes in place
- Off-label use risks include lack of individualized dosing guidance and no long-term safety data in athletic populations
For strategies that improve how peptide protocols translate into real fitness and recovery outcomes, improving peptide outcomes covers the practical variables that clinical trials don’t always address.
Pro Tip: Be skeptical of any supplement company claiming their product “activates GLP-1 receptors naturally.” This language is designed to sound scientific while avoiding regulatory scrutiny. Ask for peer-reviewed clinical data specific to their formulation. If they can’t provide it, the claim doesn’t hold up.
The uncomfortable truth about appetite peptide breakthroughs
After reviewing the facts, here’s what most guides won’t tell you about peptides and appetite control.
The clinical data is genuinely impressive. Twenty percent body weight reduction in randomized controlled trials is not a small effect. But there’s a pattern in how this research gets translated into fitness culture that deserves pushback. The numbers from trials represent outcomes under controlled conditions, with medical supervision, standardized dosing, and participants who are typically far from optimal metabolic health at baseline. Your results in a real-world context will vary considerably.
More importantly, the peptides that show the most dramatic weight loss in trials also show the most dramatic rebound when discontinued. The biology hasn’t changed. Ghrelin goes back up. PYY goes back down. The compensatory hunger mechanisms that evolved over millions of years don’t care about your six-week protocol. Sustained lifestyle change, including dietary quality, resistance training, sleep, and stress management, remains the only intervention with a strong long-term track record.
The hype cycle around peptides booming in fitness has created a market where people are spending significant money on unverified protocols while skipping the fundamentals that would actually lock in results. Peptides are tools. Powerful ones, in the right context. But a tool used without the right foundation doesn’t build anything lasting.
The most sophisticated thing you can do with this research is use it to understand your own biology better, work with qualified practitioners, and treat pharmacological intervention as a bridge to sustainable habits, not a replacement for them. The people getting the best long-term outcomes from GLP-1 therapies are the ones who used the appetite suppression window to rebuild their relationship with food, not just eat less of the same things.
Explore appetite research peptides and expert fitness solutions
If this breakdown has sharpened your thinking on appetite pathway peptides, the next step is finding resources that match the same standard of rigor. Generic fitness content won’t cut it when you’re evaluating something this scientifically nuanced.
At Primegen Labs, we’ve built our content and product approach around the same evidence-first framework this article reflects. Whether you’re starting from scratch or already deep in a peptide protocol, our evidence-based peptide benefits resource gives you the grounded perspective you need. The science-backed peptide guide is the right starting point if you want the full picture before making any decisions. And when you’re ready to evaluate specific options, our choosing peptides for fitness framework helps you apply the right criteria. Always consult a qualified healthcare professional before starting any peptide protocol.
Frequently asked questions
What are appetite pathway research peptides?
Appetite pathway research peptides are molecules that target specific hunger and satiety receptors in the brain and gut to modulate food intake, with PYY3-36 suppressing appetite via Y2 receptors in the hypothalamus being a well-characterized example.
Do over-the-counter supplements mimic the effects of prescription peptides like GLP-1 agonists?
No. OTC GLP-1 supplements lack efficacy compared to pharmaceutical-grade peptides like semaglutide, and most produce minimal clinically meaningful weight loss.
Can appetite research peptides help with genetic forms of obesity?
Yes, certain peptides like semaglutide and tirzepatide show efficacy even in genetic cases because GLP-1 analogs work independently of the MC4R pathway, which is commonly disrupted in hereditary obesity.
Are there side effects associated with appetite pathway peptides?
Yes, common side effects include gastrointestinal discomfort, and research indicates GLP-1 agonists may decrease sexual desire through serotonergic pathway interactions, among other possible effects.
How do peptides like LEAP2 and ghrelin interact in appetite control?
Ghrelin drives hunger by activating GHSR1a receptors while LEAP2 blocks the same receptor as its antagonist, and both peptides are altered significantly following bariatric surgery and major weight loss interventions.