Peptides and Immune Health: What the Science Shows

TL;DR:
- Peptides influence the immune system through precise immunomodulation, affecting cytokines and T-cell development. Their effectiveness depends on proper dosing, individual baseline health, and quality of products, with some like thymosin alpha-1 and lactoferrin having the strongest evidence. Accurate assessment, addressing deficiencies, and targeted selection improve outcomes beyond vague “immune boosting” claims.
Not all peptides “boost” your immune system. That framing is too blunt for what’s actually happening at the cellular level. Peptides and immune health have a more precise relationship than supplement marketing usually admits. These short chains of amino acids act as biological signals, influencing specific immune pathways rather than triggering a general immune surge. Research into peptide therapy for immunity has expanded rapidly, and the evidence now points to real, measurable effects on cytokines, T-cell populations, and gut barrier function. This article breaks down what the science actually says and what that means for you.
Table of Contents
- Key Takeaways
- Peptides and immune health: how they actually interact
- Key peptides with evidence for immune support
- Why dose and delivery change everything
- How to approach peptide supplementation for immunity
- Precision immunotherapy: the next frontier
- My perspective on navigating peptide immune claims
- Start with science, not marketing
- FAQ
Key Takeaways
| Point | Details |
|---|---|
| Peptides modulate, not just boost | Immune system enhancing peptides work through specific pathways, not generalized stimulation. |
| Dose changes the outcome | High and low doses of the same peptide can produce different immune cell profile changes. |
| Thymosin alpha-1 has the strongest clinical base | Approved in over 35 countries, it targets T-cell maturation and antiviral response. |
| Nutrient status matters first | Zinc and vitamin D deficiencies blunt peptide effects before supplementation even begins. |
| Emerging therapies target precision tolerance | Advanced peptide platforms aim at autoimmune regulation, not general immune support. |
Peptides and immune health: how they actually interact
A peptide is a chain of amino acids, typically 2 to 50 of them, that is too short to be classified as a full protein. That size distinction is not just semantic. Shorter chains can cross biological barriers more readily, bind to specific receptors, and degrade at different rates than larger proteins. Your body already produces hundreds of peptides that help regulate immunity, from thymic hormones to antimicrobial peptides secreted by gut epithelial cells.
When people talk about how do peptides support immune health, the answer is almost always through immunomodulation rather than a simple on/off boost. Immunomodulation means adjusting the activity and composition of immune cell populations and their signaling molecules, called cytokines, rather than just switching everything to high alert. That distinction matters because an overstimulated immune system is not safer. It’s the mechanism behind autoimmune conditions and chronic inflammation.
Immune-active peptides interact with the system through several routes:
- Cytokine regulation: Some peptides increase antiviral interferons while suppressing pro-inflammatory IL-6 and TNF-alpha.
- T-cell development: Thymic peptides influence the maturation and polarization of T-cells in the thymus and peripheral tissues.
- Gut barrier support: Certain peptides strengthen tight junction proteins in the intestinal lining, reducing immune activation triggered by intestinal permeability.
- Toll-like receptor signaling: Peptides like thymosin alpha-1 bind TLR2 and TLR4 receptors, activating innate immune surveillance.
Pro Tip: The term “immune boosting” is a marketing phrase. When evaluating any peptide for immune response purposes, ask specifically which cytokines, which cell populations, and at what dose. Vague boosting claims are a red flag for weak evidence.
Key peptides with evidence for immune support
The landscape of immune system enhancing peptides is broader than most people realize, but a few stand out because of the quality and volume of evidence behind them.
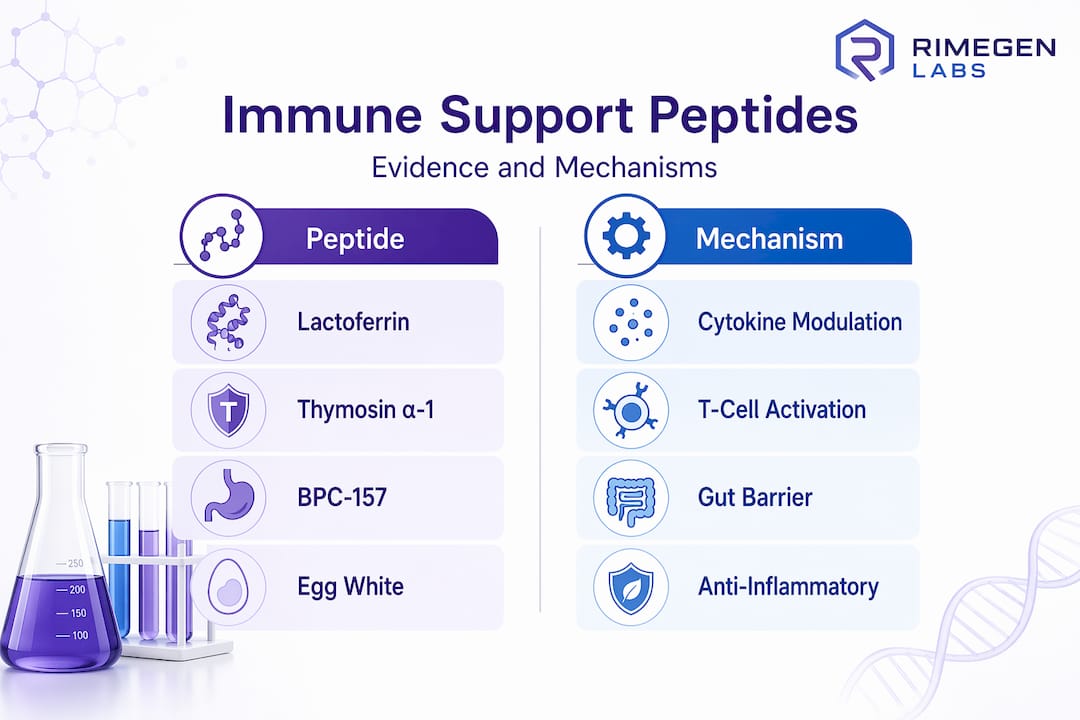
Lactoferrin
Lactoferrin is a glycoprotein peptide naturally found in colostrum and breast milk. It has been studied more rigorously for immune effects than almost any other orally available peptide. A randomized controlled trial in 103 healthy adults aged 50 and over found that oral lactoferrin at 600 mg per day for four weeks reduced IL-6 and CRP while enhancing antiviral cytokine production. The same study showed that dose determined the direction of the effect: higher doses increased total and CD4+ T cells, while lower doses reduced pro-inflammatory immune cell subsets. Two different outcomes from the same peptide at different doses.

Thymosin alpha-1
Thymosin alpha-1 is the most clinically established of all immune boosting peptides. It enhances dendritic cell activation, drives T-cell maturation, shifts the immune response toward Th1 polarization, and increases interferon-gamma production. That profile translates to stronger antiviral surveillance and improved tumor immunosurveillance. Over 100 randomized controlled trials have examined it, and it is approved in more than 35 countries for immune modulation. It is not FDA-approved in the US and is administered by injection in clinical contexts, which is an important consideration for anyone evaluating peptide therapy for immunity.
Egg white peptides
Egg white peptides are a useful example of how gut-targeted peptides produce immune-adjacent effects. An animal study found that egg white peptides improved intestinal barrier function, upregulated tight junction proteins, and reduced inflammatory pathway activity through PI3K-AKT and MAPK modulation in colitis mouse models. The caveat is real: these findings come from young mice with induced colitis. Translating them directly to human supplementation claims requires caution, but the mechanistic picture they paint is compelling.
BPC-157
BPC-157 attracts interest for gut repair and systemic effects adjacent to immunity. Its mechanisms appear to involve upregulating growth factor receptors and gut mucosal healing. Human clinical evidence remains limited, and it sits in a regulatory gray area in the US. It shows promise, but the current evidence base does not yet support confident immune-specific claims.
| Peptide | Primary immune mechanism | Human evidence level | Delivery |
|---|---|---|---|
| Lactoferrin | Cytokine regulation, T-cell support | Strong (RCT) | Oral |
| Thymosin alpha-1 | T-cell maturation, TLR activation | Very strong (100+ RCTs) | Injection |
| Egg white peptides | Gut barrier, inflammation pathways | Preclinical (animal) | Oral |
| BPC-157 | Mucosal repair, gut integrity | Limited (anecdotal) | Oral or injection |
Pro Tip: If you want the most evidence-backed entry point for oral peptide immune support, lactoferrin is currently your best option. It has human trial data, a defined dose range, and a known safety profile.
Why dose and delivery change everything
Understanding the benefits of peptides on the immune system requires confronting an uncomfortable reality: the same peptide at a different dose can produce opposite effects. The lactoferrin trial data illustrates this clearly. High doses increased immune cell counts and antiviral activity. Lower doses reduced pro-inflammatory markers. Neither outcome is inherently better. They serve different goals for people with different immune baselines.
Delivery route adds another layer of complexity. Thymosin alpha-1 is injected because oral bioavailability for many peptides is limited by gut enzymes and the acidic stomach environment. To understand this fully, you can read about peptide bioavailability strategies in depth. Oral peptides that do work, like lactoferrin, often have protective structures or are delivered in enteric formulations to survive digestion.
Individual context is equally important. Consider these variables before assuming any peptide will produce the expected result:
- Zinc status: Zinc deficiency impairs thymulin, a thymic peptide critical for T-cell maturation. A peptide protocol layered on top of a zinc deficit is working against a structural disadvantage.
- Vitamin D levels: Vitamin D insufficiency independently compromises both innate and adaptive immune responses. Correcting it first is not optional if you want meaningful results from peptide supplementation.
- Age and baseline immune status: Older adults typically show stronger responses to immune-modulating peptides because their immune regulation is already shifted. Healthy 30-year-olds may see smaller signal changes.
Most human peptide immune studies last about four weeks and measure biomarker shifts like cytokine levels and immune cell counts. Those are immunologic signals, not direct proof that you will get fewer infections. That gap between biomarker improvement and clinical outcome is real and worth holding onto when evaluating product claims.
How to approach peptide supplementation for immunity
Getting results from peptides for immune response requires a structured approach, not guesswork. Here is a practical sequence that makes sense given the evidence.
- Run baseline labs. Get a complete blood count, hs-CRP, zinc serum levels, vitamin D (25-OH), and IGF-1. Baseline biomarker testing tells you what you’re actually working with before adding any peptide. You cannot assess whether something is working without a starting point.
- Fix deficiencies first. If your zinc or vitamin D levels are low, address those before spending money on peptides. You’re not being cautious by doing this. You’re being efficient. Peptides perform better on a replete physiological foundation.
- Choose peptides with human evidence. For oral supplementation, lactoferrin has the best current profile. For injection-based peptide therapy under medical supervision, thymosin alpha-1 leads on evidence.
- Verify product quality. Peptide supplement quality varies significantly. Look for products with third-party testing and clear peptide concentration per serving. The peptide supplement science behind each product should be publicly accessible.
- Monitor and adjust. Retest the same markers at 8 to 12 weeks. If nothing has shifted, revisit the dose, the peptide type, or the underlying variables you may have missed.
Pro Tip: IGF-1 is less talked about in immune contexts, but it reflects growth hormone activity that intersects with thymic function. Low IGF-1 in older adults often accompanies reduced thymic output. Including it in your baseline panel gives you a fuller picture.
Precision immunotherapy: the next frontier
Beyond general immune support, a separate category of peptide research targets autoimmune disease specifically. These peptide-based therapeutics aim to restore immune tolerance by presenting specific disease-related antigens to regulatory T cells in a way that dials down the destructive immune attack on self-tissue. This is precision immunomodulation, and it is a fundamentally different application from taking a daily lactoferrin supplement.
The delivery technology required here is also far more sophisticated:
- Lipid nanoparticles encapsulate peptide antigens and tolerogenic signals together, mimicking the cues that prevent immune activation in healthy tissue.
- Hydrogels allow sustained local peptide release in target tissues, maintaining therapeutic antigen concentration over time.
- mRNA lipid nanoparticle platforms are being adapted to express tolerogenic peptides in situ.
The challenges are real. Epitope mapping across patients is complex because the exact T-cell targets differ between individuals with the same autoimmune diagnosis. Patient stratification remains an unsolved problem in many clinical programs. But the mechanistic clarity of this approach, where peptide immunotherapies target specific pathways and tolerance induction rather than general stimulation, represents a meaningful advance over broad immune boosting strategies.
My perspective on navigating peptide immune claims
What I have found working in this space is that most people either underestimate or overestimate what peptides can do for immunity. The underestimators dismiss the whole category because they conflate it with generic supplement marketing. The overestimators assume every peptide with an immune mechanism will visibly improve their resistance to illness.
The reality sits in a more specific place. I’ve seen the lactoferrin trial data produce genuinely meaningful cytokine shifts in older adults. That’s real biology. But I’m also aware that four weeks of cytokine changes don’t automatically translate to fewer sick days. The studies show us the mechanism is working. They don’t always show us the clinical endpoint we actually care about.
My honest take is this: peptide therapy for immunity is worth taking seriously, but it rewards specificity. If you pick the right peptide for your actual immune deficit, dose it correctly based on evidence rather than guesswork, and address your modifiable nutrient gaps first, you are working with the biology instead of against it. If you just grab a “peptide blend” marketed for immune support with no published human data, you are mostly paying for optimism.
The science is moving fast in the precision immunotherapy direction. For autoimmune conditions specifically, peptide-based approaches represent some of the most interesting clinical research happening right now. For everyday immune support, the bar should still be human evidence, defined mechanisms, and an honest read on what the data actually proves.
— Yvette
Start with science, not marketing
If this article made one thing clear, it’s that not all immune-focused peptides are equal and your results will depend entirely on which one you choose, at what dose, and whether your physiological baseline is set up to respond.
At Primegenlabs, the goal is to connect you to peptide information and products grounded in the actual evidence base. Whether you’re evaluating your first oral lactoferrin protocol or exploring more advanced options, the peptide evidence and benefits resource on the Primegenlabs site gives you the science layer that most supplement marketing skips entirely. You can also review the peptide safety guidance to make sure your approach is structured and monitored correctly from day one.
FAQ
What do peptides actually do for the immune system?
Peptides modulate immune function by influencing cytokine production, T-cell development, and gut barrier integrity rather than broadly stimulating the immune system. The specific effect depends on which peptide you are using and at what dose.
Which peptide has the most evidence for immune support?
Thymosin alpha-1 has the deepest clinical evidence base, with over 100 randomized controlled trials and approval in more than 35 countries, though it requires injection. For oral supplementation, lactoferrin has the strongest human trial support.
Do I need to test anything before starting peptides for immunity?
Yes. A baseline panel including CBC, hs-CRP, zinc, vitamin D, and IGF-1 helps identify deficiencies that would undermine peptide outcomes and gives you a reference point to measure actual changes.
Can peptides help with autoimmune conditions?
Peptide-based immunotherapies are an active area of clinical research for autoimmune diseases, using precision delivery platforms to restore immune tolerance. These are distinct from general immune support supplements and should be approached under medical supervision.
Is “immune boosting” a meaningful claim for peptides?
Not really. Effective peptide effects on immune markers are specific to peptide type, dose, and individual context. A blanket boosting claim without mechanistic or clinical evidence should be treated with skepticism.