How to Calculate Peptide Dosage: A Practical Guide

TL;DR:
- Correctly calculating peptide dosage is essential to avoid ineffective results or safety risks, relying on precise math from vial labels to syringe measurements. Using a U-100 insulin syringe and understanding your vial’s concentration ensure accurate dosing, with manual calculations helping to verify consistency and prevent errors. Proper dose planning, split dosing, and cycle lengths enhance safety and effectiveness, emphasizing the importance of accuracy and quality in peptide protocols.
Getting your peptide dosage wrong is not a minor inconvenience. It can mean zero results or, worse, a safety issue. Yet most guides skip the actual math and jump straight to “inject X mcg daily” without explaining how you arrive at that number with a syringe in your hand. Knowing how to calculate peptide dosage precisely, from reading your vial label to drawing the right amount into a U-100 insulin syringe, is what separates a protocol that works from one that guesses. This guide walks you through every step.
Table of Contents
- Key takeaways
- How to calculate peptide dosage: what you need first
- Step-by-step peptide dosage calculation
- Common mistakes when calculating peptide dosage
- Peptide dosing guidelines and cycle planning
- My honest take on peptide dosing precision
- Get quality peptides and accurate dosing resources from Primegenlabs
- FAQ
Key takeaways
| Point | Details |
|---|---|
| Know your units before anything else | Confusing mcg with mg or syringe units with mL causes errors up to 10x the intended dose. |
| Do the conversion once at reconstitution | Calculate your concentration when you mix the vial, then dose in consistent syringe units every time. |
| Label every vial immediately | Write the concentration and date on the vial the moment you reconstitute to prevent future miscalculation. |
| Split doses for better outcomes | Morning and evening split dosing improves peptide stability and biological effectiveness compared to one large daily dose. |
| Manual math beats blind calculator use | Running at least one manual calculation lets you catch entry errors before they become dosing mistakes. |
How to calculate peptide dosage: what you need first
Before you touch a syringe or open a vial, you need the right tools and a clear understanding of what the numbers on your labels actually mean. Skipping this step is where most people go wrong.
The syringe you should be using
The standard tool for peptide administration is a U-100 insulin syringe, typically with a 29 to 31 gauge needle. A U-100 syringe holds 100 units per 1 mL, which means 10 units on the barrel equals exactly 0.10 mL. That distinction matters enormously because the markings on the syringe are in units, not milliliters. If you read “10” and assume it means 10 mL, you have already made a catastrophic error.
Subcutaneous injections are the preferred route for most synthetic peptides. They reach peak plasma concentration within 30 to 60 minutes and are far easier to self-administer than intramuscular injections. For most fitness and recovery protocols, a 29 to 31 gauge, half-inch needle is all you need.
Reading your peptide vial label
Peptide vials are typically labeled in milligrams (mg) or micrograms (mcg). One milligram equals 1,000 micrograms, and nearly all dosing discussions happen in mcg. Check the total peptide content on your vial. A “5 mg vial” contains 5,000 mcg of peptide. That single conversion sets the foundation for every calculation that follows.
Here is a quick reference for the tools and items you need before you begin:
- A U-100 insulin syringe (29 to 31 gauge needle)
- Bacteriostatic water (BAC water) for reconstitution
- Alcohol swabs for sterile prep
- A permanent marker to label your vial
- Your peptide vial with total mg or mcg clearly noted
- A calculator (and the willingness to verify it manually)
Pro Tip: Label your vial the moment you finish reconstituting. Write the date, the total mcg in the vial, the volume of BAC water added, and the resulting concentration per unit. Future you will be grateful.
The volume of BAC water you use directly determines your concentration and how easy your daily dosing will be. Choosing the right amount is not arbitrary. It is part of the calculation.
| Vial size | BAC water added | Concentration per unit |
|---|---|---|
| 5 mg (5,000 mcg) | 1 mL | 50 mcg per unit |
| 5 mg (5,000 mcg) | 2 mL | 25 mcg per unit |
| 10 mg (10,000 mcg) | 2 mL | 50 mcg per unit |
| 10 mg (10,000 mcg) | 4 mL | 25 mcg per unit |
The reconstitution volume you choose directly shapes your convenience. Using 2 mL of BAC water for a 5 mg vial produces round, easy-to-measure doses. For example, 10 syringe units equals exactly 250 mcg. That kind of clean math makes daily dosing far less error-prone.
Step-by-step peptide dosage calculation
This is the actual math. Work through it once with your vial before you ever draw up a dose.
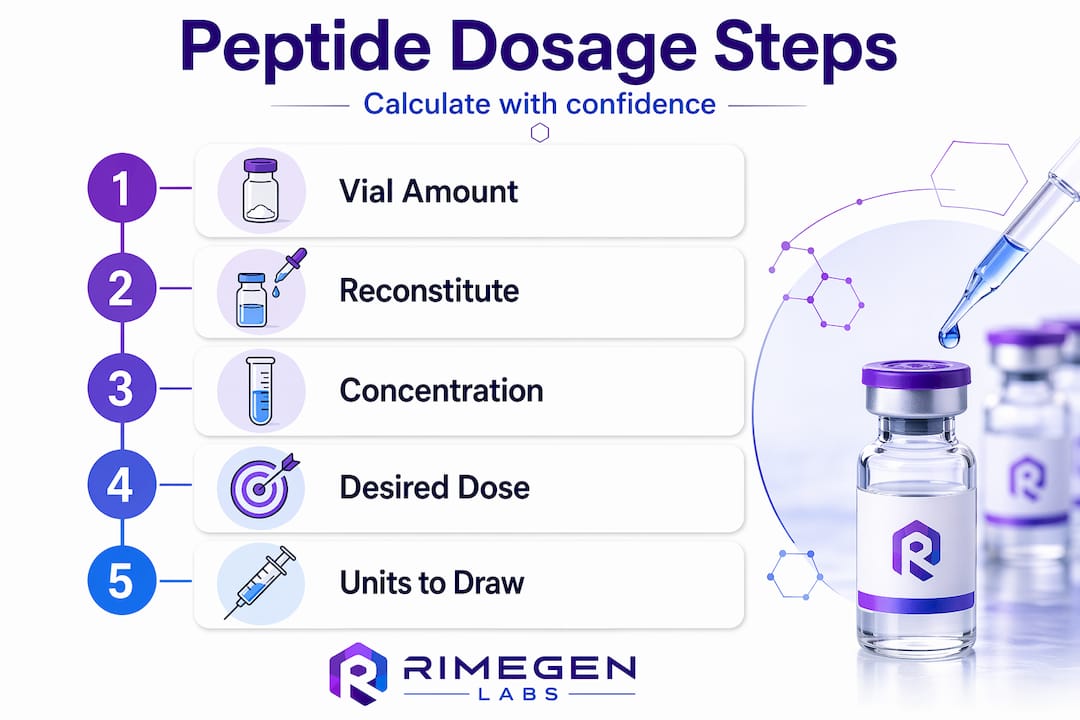
The core formula
The formula for calculating your concentration is straightforward:
Concentration (mcg per unit) = Total peptide (mcg) ÷ (mL of BAC water × 100)
Once you have concentration, finding your injection volume in syringe units is just as simple:
Injection volume (units) = Desired dose (mcg) ÷ Concentration (mcg per unit)
Work through this in steps:
- Convert mg to mcg. If your vial says 5 mg, that is 5,000 mcg. Write that number down.
- Decide your BAC water volume. Choose an amount that produces round, manageable unit doses. Two mL is a common and practical choice.
- Calculate concentration. Using the formula: 5,000 mcg ÷ (2 mL × 100) = 5,000 ÷ 200 = 25 mcg per unit.
- Determine your injection volume. If your target dose is 250 mcg: 250 ÷ 25 = 10 units on the syringe.
- Double-check the math. Multiply back: 10 units × 25 mcg = 250 mcg. Confirmed.
A worked example with two common doses
Say you have a 5 mg vial of BPC-157 reconstituted with 2 mL of BAC water. Your concentration is 25 mcg per unit.
| Target dose | Calculation | Syringe units to draw |
|---|---|---|
| 200 mcg | 200 ÷ 25 | 8 units |
| 250 mcg | 250 ÷ 25 | 10 units |
| 500 mcg | 500 ÷ 25 | 20 units |
This is the power of doing the conversion once at reconstitution. After that, every injection is just a single-step lookup. No daily arithmetic, no guesswork. You can even tape a small card to your vial with your target units marked.
Pro Tip: Use the peptide dosing guide from Primegenlabs to cross-reference your calculated doses against established protocols before you begin your first cycle.
Online calculators exist for this process, but manual calculations help you catch errors that a calculator would miss if you enter the wrong input. Run the numbers yourself at least once. If your calculator and your manual math agree, you can proceed with confidence.
Common mistakes when calculating peptide dosage
Even people who understand the formula make errors in practice. These are the ones that show up most often, and they are worth knowing before you start.
- Misreading syringe markings as mL. A U-100 syringe reads in units. Ten units is 0.10 mL, not 10 mL. Confusing units with mL is one of the most common errors and can result in a dose 10 times higher or lower than intended.
- Confusing mcg with mg. These are not interchangeable. A dose of 250 mcg is 0.25 mg. If someone’s protocol says 0.25 mg and you interpret that as 0.25 mcg, you will inject a fraction of an effective dose. If you flip it the other way, you risk a significant overdose.
- Using the wrong syringe type. Not all syringes are U-100. If you use a U-40 syringe with U-100 calculations, every dose will be off by a factor of 2.5. Always confirm your syringe type before starting.
- Skipping the vial label. Failing to label vials with concentration and date is a real problem when you are working with multiple peptides or returning to a vial after a few days.
- Not accounting for split dosing in your supply math. If your protocol calls for two daily injections of 250 mcg, that is 500 mcg per day, not 250. Planning your vial usage incorrectly means running out mid-cycle.
- Trusting a calculator without verifying inputs. Garbage in, garbage out. Entering 5 mg when you mean 5 mcg produces a wildly wrong answer.
Dosing errors with peptides are not just ineffective. They can compromise safety. The difference between 250 mcg and 2,500 mcg is a single decimal point. Treat your label and your math with the same care you would give any medical protocol.
For a solid foundation on safe peptide handling practices, Primegenlabs covers both lab prep and administration in practical detail. Getting those habits right from the start reduces every category of error covered above.
Peptide dosing guidelines and cycle planning
Understanding how to measure peptide dose is only part of the picture. Knowing how much to take and for how long completes it.
Most protocols for peptides like BPC-157 fall in the range of 200 to 1,000 mcg daily, with cycles running 4 to 8 weeks. Lower doses around 200 to 300 mcg per day suit maintenance or conservative approaches. Higher doses toward 500 to 1,000 mcg are more common for active injury repair or accelerated recovery goals.
Split doses morning and evening outperform single large daily doses for most peptides. Consistent dosing intervals support more stable plasma levels and improve the body’s response to the compound.
Here is how common goals align with dosing approaches:
| Goal | Typical daily dose | Suggested split |
|---|---|---|
| General recovery support | 200 to 300 mcg | Once or twice daily |
| Injury repair | 400 to 600 mcg | Twice daily |
| Performance and tissue optimization | 500 to 1,000 mcg | Twice daily |
Cycle length matters just as much as dose. Most peptide protocols recommend at least 4 weeks off after an 8-week dosing cycle to prevent receptor desensitization. Running a peptide indefinitely does not give you more results. It gives you diminishing returns and a potentially blunted response.
Pro Tip: Track your dosing dates in a simple notebook or app. Knowing exactly when your cycle started and when to stop is just as important as knowing how much to inject.
Injection route also plays a role in how your dose behaves. Subcutaneous delivery works well for systemic effects and is the standard for most fitness and recovery protocols. Your peptide absorption and performance can shift meaningfully based on injection site and depth, so consistency in technique matters once you lock in your dose.
My honest take on peptide dosing precision
I have worked closely with peptide protocols long enough to see a pattern: the people who get the best results are not necessarily using the highest doses. They are the ones who got the math right from day one and stayed consistent.
What I have found is that the manual calculation step is skipped more often than it should be. People copy a number from a forum, enter it into an app, and trust the output completely. But running the numbers yourself at least once makes you understand what you are actually doing. You catch things. You notice if the formula produces an oddly large or small syringe draw. That intuition only comes from doing the math.
I also think the unit confusion issue is under-discussed. People hear “microgram” and “milligram” and assume they know the difference, but under the pressure of actually preparing an injection, the decimal slips. Write it on the vial. Write it on a sticky note. Make the information impossible to forget because the cost of getting it wrong is real.
The other thing I would push back on is the idea that higher doses always equal better outcomes. Peptide dosing is not linear in that way. Receptor sensitivity, cycle timing, and consistency of administration matter just as much as the number you draw up. Precision beats volume every time.
— Yvette
Get quality peptides and accurate dosing resources from Primegenlabs
Accurate dosing math only works when you start with a quality peptide. Every calculation in this guide becomes meaningless if the peptide you are using is underdosed, impure, or mislabeled by the manufacturer. At Primegenlabs, the product selection is built around scientific backing and fitness-relevant applications, from recovery-focused compounds to performance optimization peptides. Whether you are just getting started or refining an existing protocol, the muscle growth and recovery guide gives you the context to pair your dose calculations with the right compound. And if you are ready to explore what is available, the peptide performance and benefits resource covers everything you need to make an informed choice.
FAQ
What is the formula for calculating peptide dosage?
Divide the total peptide amount in mcg by the volume of BAC water in mL multiplied by 100. This gives you mcg per syringe unit. Then divide your desired dose by that number to get the units to draw.
How many units do I draw for a 250 mcg dose?
It depends on your concentration. If you reconstituted a 5 mg vial with 2 mL of BAC water, your concentration is 25 mcg per unit, so a 250 mcg dose requires 10 units on a U-100 syringe.
What is the difference between mcg and mg in peptide dosing?
One milligram equals 1,000 micrograms. A 5 mg vial contains 5,000 mcg. Most dosing targets are expressed in mcg, so always confirm which unit a protocol uses before calculating.
How long should a peptide dosing cycle last?
Most protocols run 4 to 8 weeks, followed by at least 4 weeks off to prevent receptor desensitization and maintain effectiveness over time.
Why should I do a manual calculation instead of just using a peptide calculator?
Manual calculations let you catch input errors that a calculator accepts without question. Running the math yourself at least once confirms your concentration and injection volume are accurate before you begin dosing.